

Introduction
Clonal cytopenias of undetermined significance (CCUS) is defined by the presence of somatic driver mutations/copy number variations in hematopoietic cells in patients with low blood counts, in the absence of morphological evidence for myeloid neoplasms. Patients with CCUS are often symptomatic and can be transfusion dependent (TD), with high rates of progression to myeloid neoplasms, especially myelodysplastic syndromes (MDS). In addition, similar to MDS, there are reports of CCUS patients responding to hypomethylating agents. Due to the lack of a formal diagnosis/morphological dysplasia, CCUS patients are often denied therapies or clinical trial enrollment. We carried out this study to validate our hypothesis that CCUS shares similar clinical and survival characteristics with lower risk MDS (LR-MDS).
Methods
CCUS patients were prospectively identified from the clonal hematopoiesis clinic, whereas LR-MDS patients were retrospectively identified from our institutional database. LR-MDS was defined as very low, low and intermediate risk MDS based on the R-IPSS categorization. Baseline demographics, blood counts, bone marrow (BM) morphology, cytogenetics, and NGS results were abstracted. Transfusion dependency was defined as requiring at least one unit of red cell or platelets every 4 weeks. The Mann-Whitney-U and Fischer's exact test were used to compare quantitative and qualitative data in subgroups. Kaplan-Meier overall survival (OS) estimates were used for survival analysis and compared using the log-rank test.
Results
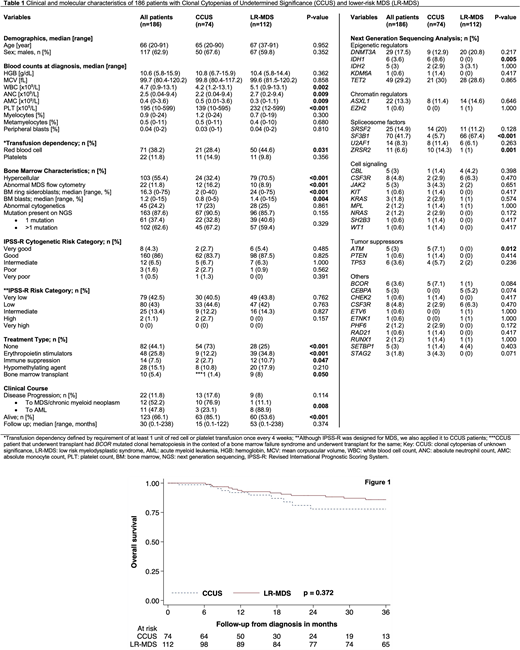
186 patients were included in the study; 74 (40%) with CCUS and 112 (60%) with LR-MDS, median age 66 years, with 63% being male (Table 1). In the CCUS group, 93% had one or more mutations (67% >1 mutation) detected by NGS, while 7% had clonal cytogenetic abnormalities. Common mutations in CCUS included TET2 (30%), SRSF2 (20%), DNMT3A (13%) and ASXL1 (11%); with 28% of patients being red cell TD and 15% being platelet TD. On application of the R-IPSS stratification, 40%, 45%, 12% and 3% were in the very low, low, intermediate and high risk categories, respectively. LR-MDS subtypes included MDS-RS (50%), MDS-MLD (21%), MDS-EB (10%), MDS del5q (7%), and MDS-U (12%). SF3B1 mutations were seen in 67% (95% of MDS-RS), while TET2 and DNMT3A mutations were seen in 29% and 21%, respectively. 60% of LR-MDS patients had >1 mutation. 44% were red cell TD, while 10% were platelet TD.
In comparison to patients with CCUS, LR-MDS patients were more likely to have higher white blood cell counts (p=0.002), higher neutrophil counts (p=0.009), higher platelet counts (p<0.001), be red cell TD (p=0.031), have BM ring sideroblasts (p<0.001), have higher BM blast% (p=0.004) and carry SF3B1 mutations (p<0.001); whereas CCUS patients were more likely to have higher monocyte counts (p=0.009) and more likely to carry IDH1 (p=0.005), ZRSR2 (p=0.005) and ATM (p=0.012) mutations. Importantly there were no differences with regards to R-IPSS cytogenetic risk groups, R-IPSS prognostic categories, platelet TD, and mutations involving TET2, DNMT3A, SRSF2 and ASXL1 and TP53. Notably signal pathway mutations and mutations involving tumor suppressor genes were infrequent (<5%) in both groups.
The LR-MDS patients had a longer median follow up (53 vs 15 months) and at last follow up 72 (64%) and 11 (15%) deaths had been documented in the LR-MDS and CCUS groups respectively. 13 (18%) CCUS patients progressed to MDS (10) and AML (3) over a median of 15 months, while 9 (8%) LR-MDS patients progressed to higher grade MDS (1) and AML (8), respectively (median follow up 53 months). There was no difference in the median survival between CCUS (median OS not reached) versus LR-MDS (median OS 8.3 years) (p=0.372, Figure 1).
Conclusion
In spite of subtle phenotypic/molecular differences between LR-MDS and CCUS, both entities had similar prognostication, distribution of high risk mutations and survival outcomes. Within a short follow-up, 18% of CCUS patients progressed to MDS/AML, indicating that regardless of the absence of dysplasia these entities are a continuum of myeloid neoplasms. In order to improve access to treatments and clinical trial opportunities, we recommend that close consideration be given to consider CCUS as a MDS subtype.
Shah:Dren Bio: Consultancy.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal